

Morgellons Disease and Elusive Treatments: A Case Study
Finding suitable treatments for Morgellons disease has been perplexing for researchers—and causing continued patient suffering—for some time. It can be challenging to pin down an infectious cause for Morgellons-like symptoms in some patients when serological testing returns false negatives.
What’s more, Morgellons disease symptoms don’t always respond well to antibiotics. This leads far too many researchers to diagnose patients with psychosis and treat them with antipsychotics with the assumption that the patient is delusional.
To better understand treatment difficulties for Morgellons disease, you’ll need to understand the pathogen causing the underlying illness, how these infecting bacteria behave in the body, and how they respond to treatment.
To shed light on a patient’s pathway to help and healing, the Charles E. Holman Morgellons Disease Foundation will present the findings from a patient case study and unfolding research surrounding Borrelia species spirochetal bacteria.
Failed Morgellons Disease Diagnosis Case Study
This case study is a typical example of how difficult diagnosing and treating Morgellons disease can be. It followed a middle-aged Caucasian female who went to a clinic in Calgary complaining of vaginal itching. She eventually developed ulcerating lesions and fiber growth throughout her body.
For three years doctors prescribed many different treatments without success.
Here’s a timeline of events:
Summer 2014
The patient experienced what she assumed was a mosquito bite. The bite was red, itchy, and cleared up more than a month later. The patient didn’t experience any other symptoms and didn’t think anything more of it.
March 2015
 The patient came to a Calgary clinic because she was experiencing vaginal itching that had lasted several weeks. Doctors discovered that her vagina and vulvar regions were red and rashy and that she also had experienced “skin loss, hypopigmentation, cracks, fissures, and ulceration” in her genital tissues.
The patient came to a Calgary clinic because she was experiencing vaginal itching that had lasted several weeks. Doctors discovered that her vagina and vulvar regions were red and rashy and that she also had experienced “skin loss, hypopigmentation, cracks, fissures, and ulceration” in her genital tissues.
Medical professionals conducted many tests, ruling out the most common STIs and bacterial infections. However, the patient did test positive for herpes simplex virus (HSV), for which she received treatment. The patient reported some improvement in her symptoms. However, she did not experience resolution of her genital fissures and ulcerations.
June 2015
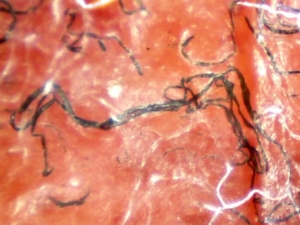
Morgellons Disease Fibers Magnified Specimen
The patient returned to the clinic because she was still experiencing painful gynecological symptoms. The patient had also developed ulcerated, punctate erosions on her back. Researchers discovered black fibers embedded in her skin during a microscopic exam under 50x magnification. These fibers pointed her physician toward a possible Lyme diagnosis.
The patient recalled being bit by an insect the previous summer and that she had developed a red, itchy rash that took longer than a month to heal. The patient thought the rash was a mosquito bite and didn’t think any more of it.
Her doctor took a blood sample and a vaginal swab to test for tick-borne infections, and the patient tested positive for a host of Borrelia species.
August 2016
The patient developed open sores on her shoulders and arms. She had been prescribed a doxycycline regimen for three months. While this treatment provided some clinical improvement, the patient’s symptoms didn’t go away. So her doctor extended her antibiotic treatment for another three months.
January 2017
The doxycycline “completely failed to resolve her symptoms” and her physician halted treatment.
Researchers studying her case conducted another series of serological testing and the patient tested positive for Borrelia species of spirochetal bacteria and several other infectious bacteria. She was placed on azithromycin and nitazoxanide therapy. The patient was able to heal completely from her lesions, regain everyday function and go back to work full time.
The patient noticed that she experienced flare-ups if she ate sugary or processed foods or was under stress.
October 2017
After breaking out in acne-like lesions on her chin, the patient returned to the clinic. She was experiencing a red, flaky perioral dermatitis-like rash around her mouth. Her azithromycin and nitazoxanide treatment had stopped and she began doxycycline therapy again.
December 2017

Painful lesions on a Morgellons patient’s legs before antibiotic treatment.
The patient’s symptoms got worse and her other symptoms returned. At this time, the patient tested positive again for infections from Borrelia and other tick-borne bacterial infections.
The patient resumed her azithromycin and nitazoxanide therapy and saw improvement for an entire year.
December 2018
The patient discontinued her azithromycin and nitazoxanide treatment, and her symptoms relapsed, developing annular rashes on her hands, legs, back, and abdomen. Her lesions grew from 1 cm in diameter to 6 or 7 cm and she also developed secondary erythema migrans rash with blue embedded fibers.
Researchers found Borrelia organisms in lesion biopsies.
As a result of clinical observations and test results, her azithromycin and nitazoxanide treatment resumed with an added short course of prednisone.
June 2018

Healing lesions post treatment
The patient’s therapy included tinidazole and trimethoprim/sulfamethoxazole, which finally resolved her symptoms. She returned to living everyday life.
The patient reported that she went back to working her full-time job and caring for her two children. Despite the gains she made in her current treatment, she did say she experienced relapses if she indulged in sugary or processed foods.
Borrelia burgdorferi
This case study shows that the patient’s use of oral antibiotics, like doxycycline, failed to resolve her symptoms and clear the underlying bacterial infection. Results like this can lead many medical professionals to believe that Morgellons is a psychiatric illness, not the result of a disease. But why does this happen when patients clearly have an underlying infection?
As it turns out, Borrelia species of bacteria, specifically Borrelia burgdorferi—the main player behind Lyme disease—adapt to living in mammalian hosts and evading both antibiotics and the hosts’ immune systems.
Special adaptations
Borrelia burgdorferi (Bb), the bacteria known to cause Lyme disease and found in 98% of Morgellons patients, is spirochetal, meaning its spiral-shaped. It has many tail-like flagella that can whip and twirl, much like a propeller, to help it move. This bacteria is fully motile or capable of spontaneous motion.
Research has found that not only can the bacteria “swim” along microscope slides, but they are actually capable of swimming through dense tissue and maneuvering through complicated cellular structures through which host immune cells are too large to travel. Bb can quite literally outrun and outmaneuver host immune cells. High motility found in Borrelia species may also account for the spirochete’s ability to move or disseminate through many different body parts and systems without using the bloodstream.
What’s more, as part of the Bb life cycle, the bacteria can regulate the genes that trigger growth in response to environmental pressures. Meaning Bb can slow growth and go dormant inside a host until conditions are right, then begin multiplying and colonizing tissues within the host.
The spirochete’s ability to go dormant explains why it may take up to a year for Lyme and Morgellons disease patients to experience symptoms after being bitten by a tick. This tendency may also account for false-negative serological tests.
Slow growth regulation also comes into play when introducing antibiotics to treat Bb infections. Antibiotics like doxycycline, azithromycin, and nitazoxanide create an unfavorable environment, triggering Bb cells to go dormant—making the infection clear somewhat and improving symptoms.
However, when antibiotic regimens halt, the environmental conditions improve so bacteria can begin growing and multiplying again—triggering more symptoms.
Please note that doxycycline, azithromycin, and nitazoxanide work by stopping the growth of bacteria so that the patient’s immune system can clear the infection. These drugs do not outright kill the bacteria.
In the end, Morgellons disease may be so challenging to treat because the bacteria responsible for the underlying infection can literally run and hide from both antibiotics and the patient’s immune response cells.
Clearly, Morgellons disease still needs more research to understand how to better combat infectious bacteria like Borrelia burgdorferi that cause so much pain and suffering for Morgellons patients.
Please donate today to help the Charles E. Hollman Morgellons Disease Foundation fund continuing research like this case study that can improve the quality of life for Morgellons patients everywhere.